MEadvocacy would like to thank advocate Eileen Holderman for her consultation on the blog post.
MEadvocacy sent a petition to NIH to cancel and restart the NIH Intramural Study on ME/CFS because of the many significant problems with the study’s design and protocol and lack of myalgic encephalomyelitis (ME) stakeholders’ input.
Since then, NIH has used various and confusing ways to communicate new and changing information about the study. As further information became available, we voiced our deep concerns about many of the significant issues with the study: multiple and ever-changing criteria, some of which are deeply flawed; biased and/or inexperienced investigators and advisors; additional problems with the study’s design; mistrust of the government health agencies and the problems with the way NIH is communicating.
This is a unique opportunity to design a robust study using the comprehensive resources of the NIH Clinical Center. It is crucial that this study be done with ME experts' and stakeholders' input from start to finish. This will ensure meaningful results and scientific advancement for patients who suffer from this serious, disabling disease.
Petition Summary
The MEadvocacy petition with 725 signatures was initiated on February 9, 2016, and sent to Dr. Francis Collins, Director of the National Institutes of Health (NIH), on February 15, 2016.
The petition called for:
-
Rejection of the Reeves’ criteria and its associated questionnaires
-
Restart of the NIH clinical study using a protocol pre-approved by ME experts and stakeholders
-
Transparent communication to the patient community
-
Use of ME criteria created by our experts to select a more homogeneous ME patient cohort such as the International Consensus Criteria (ICC) or the Canadian Consensus Criteria (CCC)
On February 23rd, we sent a follow-up reminder with additional concerns about the study:
-
NIH chose a lead associate investigator, Dr. Brian Walitt, with a psychosomatic viewpoint of the disease
-
The selection of recovered Lyme disease patient group (a disease fraught with controversy) as a comparison cohort
-
The selection of functional movement disorder patient group (a disorder that falls under the mental illness classification of somatoform disorders) as a comparison cohort
At the March 8th NIH Telebriefing, we asked a question as to when we would receive a response to the petition.
On March 11th, MEadvocacy received a reply to our petition from Dr. Koroshetz. However, Dr. Koroshetz’s reply and NIH/NINDS’ actions sidestepped our crucial concerns.
The Ever-Changing Criteria
Why is Research and Clinical Criteria Used for Patient Selection So Important in ME?
Many diseases have testable biomarkers for use in selection of patient cohorts in studies. This ensures that the correct group of patients are being looked at. This is not the case with ME. To date, a testable biomarker has not yet been accepted. Therefore, it is of utmost importance that the strictest criteria (ICC or CCC) be used in studying ME in order to ensure that investigators are looking at a homogeneous patient cohort.
Historically, the criteria issue has been a grave problem with research into ME because various vague criteria have been created and used. Overly broad CDC criteria, such as Reeves and Fukuda, include patients who have: chronic fatigue, idiopathic fatigue, somatoform disorders, major depressive disorders, and other unrelated conditions. CDC has created the problem of heterogeneity of the disease and caused the commingling of cohorts. For three decades, they have served to obscure the original findings of ME outbreaks which has led to the suffering of a million American men, women and children.
Timeline of Criteria Changes
From the time NIH posted the first protocol showing the Reeves’ criteria on their website, it has been a fiasco of continually changing criteria and news.
-
First, the initial protocol posted on the NIH website became public with what we were later told was incomplete information. This protocol showed that Reeves’ criteria would be used to select the patient cohort. Furthermore, the NIH website code reveals that changes had been made to the protocol at least two times, which makes it hard to believe that it was ‘mistakenly posted’ in order to achieve a study number, as stated by NIH (see details here).
-
Days later, the initial protocol was removed and NIH did not post a reason why it was removed.
-
Later that day, an advocate posted a notice on a website stating that NIH informed them of the following: “Enrollees will meet all definitions for ME/CFS, including Canadian Consensus Criteria, IOM, Fukuda and Reeves, in addition to post-infectious onset.”
-
A week later (about an hour after MEadvocacy’s petition was delivered to NIH), Dr. Koroshetz sent an email to a select few advocates, stating that patients will: “...qualify under multiple consensus criteria including the Canadian criteria. Reeves was being used only for stratification purposes.”
-
The next day (after Koroshetz sent his email), Dr. Nath informed the public during his CDC Grand Rounds presentation that the NIH study would use two criteria - Fukuda and CCC - for selection of patients (see slide #53 here).
-
Three weeks later, at the NIH Telebriefing, none of the four NIH presenters mentioned criteria. However, it was announced that a new website for the study went up that morning which shows one specific criteria to be used - the CCC (item #1 on FAQ page).
-
The most recent letter to MEadvocacy by Dr. Koroshetz now states that two criteria - the CCC and IOM will be used for selecting patients (3rd paragraph).
The Need for Real ME Experts in the Study
In his March 11th letter to MEadvocacy, Dr. Koroshetz states: “As you may know, the NIH study protocol is still being revised. It is being developed with guidance by experts from a number of disciplines and is intended to be the most detailed physiological analysis to date of patients who developed ME/CFS following an infection.”
Dr. Koroshetz sidesteps our request for ME experts and patient advocate involvement with the study design and protocol from the beginning. He responds with the information that experts from a number of different disciplines were involved in the guidance, but doesn’t state that they were experts specifically in ME.
If ME advocates would have been involved from the beginning and given power of approval, Drs. Brian Walitt, Fred Gill and Leorey Saligan would not have been put in charge of assessing diagnostic validity for selecting and managing patients in the clinic.
The Inherent Bias of the Lead Associate Investigator and Those in Charge of Patient Selection
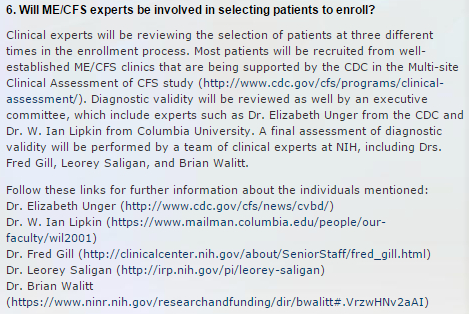
The FAQ section of the NIH study website states the following: “Most patients will be recruited from well-established ME/CFS clinics that are being supported by the CDC in the Multi-site Clinical Assessment of CFS study.”
It says “most” but not all. This is very troubling because we don’t know what they mean by “most”. For instance, does it mean 25 patients will come from the ME/CFS clinics and 15 will not? Where will those not coming from the ME/CFS clinics come from? Furthermore, the website instructions state that one can register online to become a participant in the study. Where are those patients coming from?
The final assessment will be done by “clinical experts at NIH, including Drs. Fred Gill, Leorey Saligan, and Brian Walitt” who have inherent and common biases about the disease. We do not believe the selection of these specific NIH researchers, who have the same inherent bias, is a coincidence, but rather an indication of the path this study was intended to take.
{kind=link}
NIH Intramural Study on ME/CFS website - FAQ section
Dr. Brian Walitt has been selected by NIH as lead associate investigator for the study, as well as part of the committee selecting the patient volunteers. Much has already been written about the concerns of having a lead associate investigator who believes fibromyalgia and chronic fatigue syndrome (CFS) are psychosomatic and somatoform disorders. In September 2015, Dr. Walitt gave an interview at a rheumatology conference on fibromyalgia which advocate Jeannette Burmeister blogged about. It is troubling that Dr. Walitt will be responsible for administering the subjective questions/questionnaires by phone and in person at the clinic.
Below are just a few studies Walitt has been involved with:
-
Quantifying the influence of child abuse history on the cardinal symptoms of Fibromyalgia
-
What Is Fibromyalgia, How Is It Diagnosed, and What Does It Really Mean?
Dr. Fred Gill worked with the late Stephen Straus, NIH virologist who ignored the biological evidence of ME in favor of a psychological view which set the tone for decades to come, as noted by advocate Dr. Mary Schweitzer in her blog. In a letter (part 1 and part 2) Dr. Straus wrote to Dr. Fukuda, he laid out his plan to “evaporate CFS”; see advocate Craig Maupin’s blog, The CFS Report.
{kind=link}
{kind=link}
In February 2011, Dr. Gill presented at NIH (presentation video here at the 54:17 minute mark) he said: “Dr. Straus who was much younger than me and not with us anymore but my mentor in EBV and Chronic Fatigue finally wrote a paper near the end in 2004 about pharmacotherapy. All the things I just showed you. And I agree with what he said to this day that many therapies have been tried but so far only cognitive behavioral therapy and graded exercise appear to be meaningful, to produce meaningful benefit.”
Advocate Charlotte von Salis attended the presentation and blogged about it here. What follows is an excerpt from her blog: “Gill’s big on reassuring the patient, avoiding unnecessary tests, avoiding debate over whether it’s psychological, and above all, getting patients to remain active and exercise no matter what.”
Dr. Leorey Saligan is a family nurse practitioner/investigator who researches biobehavioral mechanisms of fatigue. He states that the reason that CFS patients report pain and fatigue is because they seek attention and are catastrophizers.
Below are just a few studies Saligan has been involved in:
-
Quantifying the influence of child abuse history on the cardinal symptoms of Fibromyalgia
-
Beyond pain in Fibromyalgia: insights into the symptom of fatigue
Ways to Correct Problems with the Criteria and Investigators
-
Use a single criteria for the study - the ICC or the CCC.
-
Declare officially that NIH will not use the Reeves’ criteria and questionnaires (see references 11, 13 and 14) for any purpose in the study (see here for concerns about Reeves’ questionnaires). Replacement questionnaires (aka ‘instruments’ per clinical investigators) must be approved by ME experts and stakeholders.
-
Remove Walitt, Gill, and Saligan from the study and replace them with individuals with knowledge of ME as a biomedical disease who currently and historically do not ascribe to the psychosocial or psychosomatic causation of symptoms.
Problems With Executive Committee Advisors Who Are Not Experts In ME
Dr. Elizabeth Unger, CDC virologist, focused many of her studies and presentations on fatigue and the mind/body theory as she explained in this CFSAC video clip (posted by advocate Khaly Castle). As co-author of the Reeves' criteria, Dr. Unger explained in this video how her agency applies the criteria when asked by Eileen Holderman, former CFSAC Member, how CDC plans to reconcile the case definition issue. In the NIH study, Dr. Unger has been assigned to the executive committee and charged with reviewing diagnostic validity of the patient cohort. At the February 16th CDC Grand Rounds, Unger promoted graded exercise therapy (GET) and cognitive behavioral therapy (CBT), which is also promoted by the PACE Trial, for which ME experts have warned against as causing harm to patients.
Below are just a few studies Unger has been involved in:
Dr. W. Ian Lipkin is a world renowned virologist. In recent years, Dr. Lipkin has been investigating ME/CFS and collaborating with ME experts. Dr. Lipkin serves as an advisor on the study and will approve patient cohort selections. While Lipkin’s research shows great promise, he is not an expert in diagnosing and treating ME patients.
Ways to Correct the Problem with Advisors Without ME Expertise
-
NIH should seek advisors to the executive committee that have extensive experience investigating, diagnosing, and treating ME patients.
-
Advisors need to be approved by ME stakeholders.
Additional Problems with the Study’s Design
-
The cohort size of 40 ME patients is too small.
-
The study excludes patients who are the most severely affected such as the homebound and bedbound.
-
The use of recovered Lyme disease comparison control groups will obfuscate the results.
-
The summary of the study states they will conduct a bike exercise test twice, but does not specifically state the consecutive two-day CPET testing for post-exertional neuroimmune exhaustion.
-
The specific budget for this study has not been released and published.
Ways to Correct Problems with the Study’s Design
-
Increase the ME/CFS patient cohort size to increase probability of producing meaningful statistical results.
-
Include homebound and bedbound patients in the study. Historically, these patients have been under-researched and have the greatest potential to yield strong biomedical abnormalities.
-
Remove the asymptomatic recovered Lyme disease comparison control group from the study because they are prone to developing chronic Lyme disease (refer to here and here). In addition, the 2-tier testing used by the CDC for Lyme disease is not accurate. ME and chronic Lyme disease have overlapping symptoms and many ME patients are undiagnosed chronic Lyme disease patients due to a high level of false negative CDC test results. Therefore, this would obfuscate the comparison of these two disease groups.
-
Incorporate the consecutive two-day cardiopulmonary exercise testing (CPET) protocol into the study. The current bike exercise test, mentioned in the study summary, does not confirm whether post-exertional neuroimmune exhaustion occurs by documenting reduced VO2max on the second day.
-
Release and publish all budget information regarding funding for the study from its inception to conclusion.
Mistrust of Government Health Agencies and Problems with the Way NIH Communicates
The government health agencies have a history of malfeasance with this disease as documented by journalist and advocate Hillary Johnson in her book Osler’s Web. In 1985, the CDC went to Lake Tahoe, Nevada to investigate an ME outbreak and dismissed what they saw. They renamed the disease with a trivial moniker, chronic fatigue syndrome (CFS), and created a vague definition - both of which have caused serious harm to patients.
Additional abuses to the ME community include: CDC diversion of $12.9 million earmarked for ME/CFS research to other diseases; NIH underfunding biomedical research; Chronic Fatigue Syndrome Advisory Committee (CFSAC) FACA violations; HHS threats of eviction made to three CFSAC members; NIH/HHS FOIA violations and unreasonable conduct during the trial of FOIA violations (refer to Jeannette Burmeister’s blog on violations); and HHS dissemination of erroneous information about the disease to medical professionals, the media, and the public.
As illustrated, the patient community is justified in their mistrust of the government health agencies. Therefore, the burden is on the health agencies to rebuild the lost trust. NIH’s miscommunications are contributing to the mistrust.
Problems with the Way NIH is Communicating
-
Causing confusion by posting the intramural clinical study summary on clinicalstudies.info.nih.gov and clinicaltrials.gov websites then deleting the information (study numbers 16-N-0058 is the unofficial archive of original summary from clinicalstudies.info.nih.gov and NCT02669212 is the official archive of linked study on clinicaltrials.gov). Removing the initial study from the websites concealed the historical changes made to the study. Creating a webpage connected to the Trans-NIH ME/CFS Research Working Group describing the study. Creating another website for the NIH Intramural Study for ME/CFS.
-
Communicating information and conducting private meetings to only a select few advocates instead of the entire ME community.
-
Conveying conflicting information (by various agencies) about the study by various websites, presentations, and communications.
-
Sidestepping advocates’ questions and concerns (see examples below).
-
In his reply to advocate Joni Comstock’s question during the NIH Telebriefing, Dr. Walter Koroshetz stated: “ ...our intent is to reach out and get input from a wide variety of folks with expertise and with experience in this illness. And we have been doing that right from the beginning at NIH through the Trans-NIH Working Group, through the CFS Advisory Committee. We’ve had multiple meetings with experts in the field and with advocacy groups. And I must say it has been a challenge for us because there are, well we may not have reached out to everybody.”
Does “experts in the field” mean ME experts? NIH has not officially notified the community about specific ME researchers, clinicians or advocates who have been advising about the design of the study. There have been no assurances that ME experts and their input would be part of the study’s design and approval process.
-
Dr. Koroshetz further states: “And so, I think that the major teachers at the NIH really have to be the patients who have made the sacrifice to join the protocol, to come into the Clinical Center and to work with the doctors.”
By the time patient volunteers are involved, the design and protocol for phase 1 will have been set. Clearly, ME experts’ and stakeholders’ input and approval will not be be considered.
-
At The CDC Grand Rounds (You Tube video minute mark 53:23), Dr. Nath stated: “So, careful listening to patients is absolutely critical. So, with that in mind, you know I grew up in the early AIDS epidemic, and I saw interactive with Act Up, and other patient forums whereby they had a great impact on the way disease was handled, treated and moved the Federal government to make changes at every level. And so, we understand the importance of it, and there are efforts under way to put that advisory group together.”
Yet, at the NIH telebriefing, Dr. Nath stated: “So we looked into some of the legalities about patient advisory groups and it’s a little bit complicated in the federal government.” This implies that the assurance made by Dr. Nath at the CDC Grand Rounds regarding creation of a patient advisory group to provide input on the study may not occur because NIH does not want to deal with looking into an important but possibly complicated matter.
On one hand, NIH is telling the community they want patient and advocate input but on the other hand, NIH is implying that patients should just stick to telling them about their symptoms rather than advise them about the design of the study.
Ways to Correct the Problems with the Way NIH is Communicating
-
Reinstate the original protocol on http://clinicalstudies.info.nih.gov/ and clinicaltrials.gov, showing the changes that have been made. Also, remove the now inaccurate Trans-NIH Research ME/CFS Working Group “Eligibility Requirements for ME/CFS Clinical Study at the NIH” orphan webpage that still references functional movement disorder as a cohort. Release the history of the protocol to the public including protocol details and the Institutional Review Board (IRB) approval dates so that appropriate ME stakeholder input can be provided.
-
Communicate all information in real time to the entire community by using an NIH ME/CFS listserv.
-
Coordinate information across various agencies and sources so that all messaging is consistent.
-
Initiate and maintain a transparent and two-way communication process between NIH and the ME community (researchers, clinicians, advocates and patients) at every step of the study.
NIH Needs to Step Up!
For over 30 years, NIH and CDC have had a history of institutional bias, malfeasance and medical abuse toward the ME community. They have accomplished this by creating a trivial name and erroneous criteria, underfunding, and the promoting of harmful treatments such as GET and CBT. The Department of Health and Human Services (HHS) has ignored our ME experts’ biomedical evidence of abnormalities in the neuro-endocrine-immune systems of patients with ME - and instead used their own psychosocial and psychosomatic theories to describe a serious neuroimmune disease.
HHS needs to make concrete changes in order to affect real change in how ME is perceived and studied. Although NIH deems this study as only one piece of the puzzle, the Department has a record of turning that puzzle piece into a cornerstone of research dogma for decades to come.
Because of the opportunity for great discovery using the comprehensive resources that the NIH clinic has to offer, it is this very reason, we call for NIH to restart the study and include ME experts’ and stakeholders’ input throughout the entire process. The NIH study needs to use one criteria (the ICC or CCC), remove investigators and advisors without ME/CFS expertise and/or who possess a psychological bias (such as Drs. Walitt, Gill, Saligan, and Unger), eliminate comparison groups that will obscure study results, and communicate transparently to the entire ME community.
Now is the time for NIH to stop sidestepping the critical concerns ME stakeholders have about the study and step up to make the changes called for!
*Please note: MEadvocacy uses the term myalgic encephalomyelitis [ME] to describe the disease defined in the ICC or CCC. When we use the term ME/CFS or chronic fatigue syndrome [CFS], we are using the terminology due to the specific context in the blog. For information see www.MEadvocacy.org.
For Further Facts About ME, see MEadvocacy’s
Showing 26 reactions
Instead, the NIH has loaded this study with investigators who believe ‘Chronic Fatigue Syndrome’ is some kind of psychosocial chimera. The jesuitical equivocations of Dr. Brian Walitt are really mind-boggling. He believes that ‘all experiences are psychosomatic’. He has asserted that society, patient advocates, misguided physicians, and those alluring disability benefits account for the phenomena of this latter day neurasthenia. This is incredibly insulting to those of us who have had virtually everything taken from us, and have to cope with the frustration and grief of being unable to do the things we need to do and would love to do. Every M.E. patient I know was gainfully employed (often in careers for which they had specifically prepared, with a lot of hard work), had a reasonable expectation of making a decent living over their lifetime, and often, had many other interests that they enjoyed pursuing. As for the benefits, is he serious? Many of us reach the point of being unable to heat our homes (some are living with relatives, or in cars), and wondering if cat food, spread on a little toast with some lettuce, might be palatable. This on top of the enormous physical suffering this disease brings. Only a very cynical human being could either propose, or believe, such theories.
To me, the most glaring fault of the NIH study is the complete absence of anyone with expertise (especially clinical expertise) in M.E. My own doctor is an actual expert. In contrast with the rambling, unconcerned musings of Dr. Walitt, she has warned me about my increased risk of cancer due to my immune system being so compromised. If the NIH were actually serious about helping M.E. patients, they would call on researchers with proven track records in the science of this disease. I am alarmed and angry at the way this is shaping up.
Patient desires and needs are being overridden by the selfish goals of the phony “advocates” and fake “patient” organizations who are promoting this study. If ME patients want progress in ME research and treatment, now is the time to make our desires known. When this bogus NINDS study is under way, it will be too late. The time to act is now! If we do not do something now, this NINDS study will be PACE on steroids and it will affect ME patients all over the world.
I have said it so many times before—feels like thousands of times—the NIH does not care one whit for what the IOM report says. They do not have to follow anything it says and they have no intention of doing so. They are setting up this bogus “study” to be the US version of the PACE trial so they can recommend CBT and GET for ME patients and prescribe antidepressants and pain meds so their big pharma friends can make money off ME patient misery. And so NIH can hide the epidemic of ME for ANOTHER 30 yrs. If ME patients do not want another 30 yrs of misery and death, now is the time to make some noise!
If you are concerned about this bogus NINDS study, the first thing to do is say publicly wherever you can—anywhere on the internet—that your protest the study. Post your thoughts on your facebook page and share it in any groups you can. If you are on twitter, then tweet your opposition. If you are a member of any forums, post your opposition to the study there. and always use tags such as #PACEonSteroids Those phony “advocates” and fake “patient” organizations say they speak for ME patients. We need to let the #NIH and #CDC know they do not speak for us. They are busy telling CDC and NIH what they want to hear and our government agencies will not know the truth unless we tell them. So let’s tell them—loud and clear—WE PROTEST THE BOGUS NINDS study!
Here are some people to tweet to: @nihdirector @secburwell @drfriedencdc @plzsolvecfs @pandoraorg @meactnet @cortjohnson @sjmnotes @jenbrea @brianvastag
We need to speak up loudly and clearly or all the NIH and CDC will hear will be the cooing adoration of their toadies! So, first go write a comment on Jeannette’s blogpost.
http://thoughtsaboutme.com/ She is speaking up for us!
Post your comment here on ME Advocacy Org expressing your concern about the study.
If you can’t be bothered to post a sentence or two in support of those who are questioning this study, then you are falling into the trap of silence, which has given ME patients 30 years of contempt and neglect from medical professionals and our governments. Do you want another generation of this mistreatment. If not, now is the time to speak up!
Of course the toadies will try to shut us up. They want NIH and CDC to believe they speak for us and they tell us what to do. We need to make it clear to everyone that they do not speak for us and they do not tell us what to do! We speak for ourselves and we make our own decisions!
Patricia Carter
From a reading of this review it is apparent the study has many irredeemable flaws. Well done to MEAdvocacy for holding the NIH to account and for standing up for patients.
where Dr. Cheney uses the term “chronic fatigue syndrome”
https://scontent.xx.fbcdn.net/hphotos-xap1/v/t1.0-9/10376192_10153501095676188_2398317394061841333_n.jpg?oh=2bb7d12bcaedc3397a844758fec592ac&oe=578B34CA
For what it’s worth, the now deleted NICCH page said: “Dr. Walitt has a dual role as a medical officer at the National Institute of Nursing Research.”
Those who might not know who Straus was (he died in 2007 of brain cancer) – he was our Simon Wessely. Straus was at NIAID (National Institute for Allergies and Infectious Diseases) and considered himself the national expert on Epstein-Barr. He made headlines in the mid-1980s when he declared the mysterious outbreak of disease around the country to be “Chronic Epstein-Barr Virus” (or CEBV) because in many cases it began with EBV.
He ran some studies with IV gancyclovir, which was a much more dangerous drug than the oral form – in particular, you must protect the kidneys. He failed to hydrate the patient properly, and consequently fried some patients’ kidneys. (I knew someone who lost a kidney to the study.)
At this point Straus decides it is NOT CEBV, that in fact it has nothing to DO with EBV (He was also informed by the research community that 90 percent of American adults test positive for EBV). In 1986, Straus submitted a request to NIH for funding to continue his work on CEBV – except he wanted to use the name “the chronic fatigue syndrome.” That is the earliest use of the term we have been able to find – and if anybody knows an earlier use, please let us know!
When the Holmes committee met, the new name that was supposedly invented at the meeting was pre-ordained, because Gary Holmes (of CDC) and Steve Straus were running the show. Around 4 researchers familiar with M.E. tried to convince the group that these outbreaks were actually M.E., but they were voted down. As a scholar, I am dismayed that the suggestion did not at least find its way into a footnote IN CASE WE LEARNED SOMETHING LATER! But that would only have blurred things, so they didn’t include any mention of it.
So if you actually look at the Holmes article (1988), you’ll find that the name “chronic fatigue syndrome” was created NOT to replace M.E. (not in use in the US anyway), but explicitly to replace CEBV.
Now here’s where it gets a bit odd. When the Holmes definition was published, Straus published a different piece – rather a companion piece – that went into the history of the disease. in THIS article he DID acknowledge the link to atypical polio from 1934, the various names, particularly Islandic Disease, and THEN he added
Epidemic Neuromyesthenia
Why that’s odd, is that epidemic neuromyesthenia was the name Americans chose then the UK (and Canada and Australia) adopted myalgic encephalomyelitis, in the mid-1950s, when the polio vaccine appeared to put an end to polio. So while M.E. was emphatically rejected by the Holmes/Straus meeting that led to the Holmes definition (1988), Straus showed clearly that he knew very well that these outbreaks could be M.E. – except he used the American term, which had fallen out of usage.
The last paragraph of the article was the most curious – he said that it was well known that patients with CFS were a bit neurotic. For that he cited two articles from 1970 and 1971 by psychiatrists McEvedy and Beard, claiming that M.E. was really mass hysteria (using two examples where it broke out in women’s dormitories – one of which was the Royal Colleges outbreak). He also cited “American Nervousness” (1869) a truly bizarre book that Wessely would also cite as the origins of the term neurasthenia – it turned out that while mass hysteria was not looked upon very seriously, they could get away with neurasthenia (even if they had to use a book written in the same decade of the Civil War).
At this point Straus became very angry with patients – he had become persuaded the disease was psychiatric in origin and that we were obstacles in understanding it because we just refused to admit it was psychiatric. Same as Wessely’s tune, though he emphasized stress (especially the stress of being an upper middle class white woman trying to “have it all”).
Straus was NOT a psychiatrist or a psychologist and he was still based at NIAID (National Institute of Allergies and Infectious Diseases). If he was right, why wasn’t it moved to NIMH (National Institute for Mental Health)? That question has never been answered.
However, he spent the rest of the 1990s denying numerous requests for funding for biomedical evidence concerning ME/CFS.
Straus’ boss, Anthony Fauci, came to NIAID in 1983, and was part of the AIDS coverup before being a major player in the ME/CFS coverup. And he thought Straus was a genius. When Straus died, he showed up at a meeting with patients to express his condolences for the loss of a man we surely considered a hero. (really?)
In 1999 Straus’ reputation as a shooting star led to his being named the Director of the newly created CAM (Center for Alternative Medicine) at NIH – which appears to be where psychobabble has gone to live, since NIMH doesn’t want it. Straus headed CAM until 2006; he died in 2007. I do not know how long he was able to really function there; it depends on how slow-growing the brain cancer was. But he was technically in charge until 2006.
CAM was formally renamed the National Center for Complementary and Integrative Health, or NCCIH. But they still call it CAM.
One wonders how much influence Straus had over the internal projects at CAM – Walitt’s link there does seem a bit unfortunate. One also wonders why Walitt was at NCCIH (CAM) until late last year when he was suddenly shifted over to NINH (National Institute for Nursing Health).
Fauci is still at NIH; perhaps he was aware of Walitt’s research.
But what’s very interesting is that Walitt’s profile at NCCIH, which I looked at a couple of days ago … is gone. All the references say NINH.
Curiouser and curiouser.
However, it is overwhelmingly unlikely that Walitt’s role is limited to paper pushing. He, after all, got a special shout-out by Dr. Nath during the CDC Grand Rounds presentation for his “valuable advice” in refining the study. Nath didn’t mention any of the other 26 or so investigators who are part of the study.
In the recent tele-briefing on the study, NIH trotted out Collins, Koroshetz, Whittemore, Nath and Walitt who was prominently featured on the call. Aside from Nath, the PI, and Walitt, none of the other investigators were on the call.
Walitt’s initial title was that of “lead clinical investigator,” which interestingly later, after a huge outcry by patients, was apparently changed to “lead associate investigator”—a downgraded title that seems designed to imply less authority and, hence, less of a threat to the patient community.
Most important, however, is the following. This is how Walitt’s role at NCCIH was described on its website:
“As Director of Clinical Pain Research for the NCCIH Intramural Laboratory of Clinical Investigations, Dr. Walitt will provide his medical and scientific expertise to the development and oversight of intramural clinical protocols. He will help identify patient populations for pain studies …"
So, Walitt’s role at NCCIH has been as follows:
That quite clearly is a central role as an investigator that goes far beyond that of a paper pusher with merely administrative duties.
If you add up Walitt’s special title in the “ME/CFS" study (even the downgraded one), the special acknowledgment by Nath of Walitt’s role in developing this study, Walitt’s prominent participation in the recent tele-briefing and his NCCIH responsibilities, it simply leads to the unavoidable conclusion that Walitt is going to have a major and critical role in the “ME/CFS” study.
I copied the above NCCIH website language from the following link:
https://nccih.nih.gov/research/intramural/laboratory-clinical-investigations-branch/staff/walittb
This was a working link only three days ago; it no longer is. Now, the URL returns “Page Not Found.” It incorrectly states that the page was last modified on February 12, 2015. I suppose it is possible that Walitt is no longer with NCCIH and that that is why his bio was removed, so recently.
Walitt’s position at NCCIH (National Center for Complementary and Integrative Health) is, of course, of huge concern. NCCIH was originally NCCAM (National Center for Complementary and Alternative Medicine). NCCAM’s first director (in 1999) was Strauss!
You may want to say more about Strauss and NCCAM, Mary.
1. The expert committee contains 4 people out of 5 who are bad choices for “experts.” Two have stated outright that the disease is a type of somatoform disease and/or that it is caused by catastrophizing (thinking about being sick); two are still committed to CBT/GET (i.e., patients need counseling and exercise to get better). Gill has been too far away from the literature from too long and does not understand the disease well. Unger believes the CBT/GET literature (which is about somaticizing) is “scientific.” Walitt as recently as last year published an article where he used chronic fatigue syndrome as an example of a somatoform disorder; and Saligan has published studies claiming that patients have a lot of pain because they “catastrophize” – worry about having pain (because the two are correlated); he has recently shifted to using the same model with patients who are “fatigued” – Saligan’s model that correlation is causation would be shot down in a Statistics 101 course.
I believe there is absolutely no excuse for Walitt or Saligan to have anything to do with the study. Indeed, I do not understand WHY they have anything to do with the study. I have been told backchannel that they won’t really be able to impact the study; they’re just going to be filling out applications and questionnaires and such. If so, then you can pick anybody from NIH who has no preconceptions about this disease and let THEM do that job. Better yet, we’ll train somebody from NIH to replace them. But they should be having nothing whatsoever to do with patients with ME/CFS.
In the 30 years this disease has been ignored – while a million American adults (and the number is increasing) have suffered from it – people like Walitt and Saligan ARE THE PROBLEM.
2. I understand there is only enough money to study 40 patients and that will take a year. I do not understand WHY there is only enough money to study 40 patients and that it will take an entire year to do so. Again – ONE MILLION PATIENTS IN THE US, with 500,000 unable to work AT ALL; best estimate at least 250,000 bedridden and/or housebound. People are dying from this disease; more and more people get this disease every year. What part of “urgent” does NIH still not understand?
3. The Reeves definition basically consists of a series of questionnaires. Dr. Unger was a co-author on the publication introducing those questionnaires. I am concerned that the Reeves definition will remain in the study if the questionnaires are used without the PIs knowing that the QUESTIONNAIRES are what we mean when we say the REEVES definition.
All this could be avoided by an open meeting in person with patients and specialists; by working with CFSAC; by listening to the community. Isn’t that what happens with AIDS? Isn’t that what happens with breast cancer?
As the founder of a local support group, I hear story after story of patients unable to find doctors who know how to provide care for anyone with ME. Recently, I was told by a patient leaving a doctors office devastated because the doctors response was “I don’t believe this is a disease”. Others are told they need to exercise which leads to a worsening of their health and bewilderment by the doctors as to why their patient is getting sicker. The science is clear that exertion exacerbates this devastating illness and yet doctors have not been educated about the dangers.
Any study MUST include post exertional neuroimmune exhaustion in the design and screening of patients.
It is shocking that standards at the NIH, the nation’s primary medical science research organization, have fallen to this abysmal level when dealing with the long-neglected neurological disease myalgic encephalomyelitis. The leadership at NIH has sadly chosen to accept unquestioningly the failed, fatigue-based approach to the disease promoted by the CDC that has stifled progress in ME research and treatment for three decades.
US ME patients have waited 30 years for their government to sponsor some positive, rational, and useful research on the disease. Instead we get only more politically controlled, hopelessly muddled, wasteful pseudoscience from the NIH and CDC. Until their institutional bias can be addressed and overcome, it would be better to have no research at all on ME from these organizations than the creation of more confused and biased medical misinformation purporting to be science-based.
I believe any new research on ME must build on existing unbiased research and unambiguous selection of subjects who actually have the disease being studied. Research on other neurological diseases, such as multiple sclerosis and Parkinson’s disease, is conducted on subjects with those diseases, rather than subjects with an ill-defined fatigue syndrome. People with ME should expect and accept nothing less from their government medical research organizations.
The NIH personnel involved with this study and any aspect of addressing the diseases known as ME and CFS should absolutely read and try to both understand and address the situation. Reliance on a self-referential assertion that bias can’t exist at the NIH denied a harmful history and a very threatening present course of action.
The patient population certainly deserves and should demand the respect and consideration of the researchers involved. The NIH needs to contact with actual clinical experts, not individuals like Walitt who, unless he retracts every paper he’s published stating that “cfs” is a somatoform disorder, should immediately be removed from all present and future work on this disease.
Every single patient I know has had incredible difficulty obtaining appropriate medical care because of the decades of misinformation coming partly from the NIH and leading to a habit of neglect, stigma, and mistreatment. If they have actually changed their course, the National Institutes of Health will prove that by giving the knowledgeable researchers, clinicians, and patients power to shape this crucial work. Lip service and group phone calls in which legitimate concerns are denied will not do.
It is hard not to be amazed by the continuing change of the criteria for the cohort selection, which you have so effectively laid out. From (1) Reeves only to (2) CCC, IOM, Fukuda & Reeves to (3) unspecified multiple criteria (http://www.nih.gov/mecfs/eligibility-requirements-me/cfs-clinical-study-nih) to (4) multiple criteria including CCC to (5) Fukuda & CCC to (6) finally—for now—CCC & IOM. NIH has so far revised the criteria five times, that we know of. If the agency needed any indication that it should have involved patients and true experts from the start, this sad display should suffice.
Let’s take the IOM criteria, for example. They were supposed to be clinical diagnostic criteria only. The IOM committee members went out of their way to stress that developing research criteria was beyond their charge and it, indeed, was, according to the IOM Statement of Work/Request for Proposal. That is of utmost importance because the IOM criteria do not contain any exclusions of other fatiguing illnesses, which, in a research setting, spells disaster. Diluted research cohorts inevitably lead to perversely distorted “science,” the last thing our community needs, deserves or can absorb.
Here is the problem. Although the IOM committee members emphasized that they had not created a research definition, they not only failed to expressly include instructions, in the IOM report, that the new criteria not be used in any research, they even inconsistently encouraged the use of their new criteria in research:
“Future diagnostic research will be most instructive when protocols include patients identified using the committee’s proposed diagnostic criteria for ME/CFS as well as patients with other complex fatiguing disorders. Almost all of the studies conducted to date have compared patients with ME/CFS with healthy controls rather than with patients with these other fatiguing disorders.”
And that is exactly what is happening with the NIH study.
Please note the encouragement of the IOM to study our disease together with “other fatiguing disorders” as control groups, as if fatigue is the defining symptom of our disease. That reminds me of Dr. Collins’ musings, in his Charlie Rose interview, that this study might lead to answers about questions on fatigue in cancer and also of the fact that NIH considers, for the comparison group of the study, post-Lyme patients to be asymptomatic when they no longer experience fatigue. With its (Reeves?) fatigue questionnaires and diaries, the initially published requirements that fatigue have started after an infection and have lasted more than six months, etc., this study has fatigue written all over it. Never mind that fatigue is not the defining symptom of our disease.
In a study where the CCC with its exclusions are also used, the IOM criteria’s lack of exclusions is mitigated. But what is to keep somebody like Wessely from using the IOM criteria in the future without the checks and balances of the CCC? Nothing. What’s good enough for NIH will surely be good enough for, well, everybody else. Using the IOM criteria in this study will send a precedent for future research that is liable to have far-reaching and devastating consequences.
In terms of the two-day CPET, NIH has recently sent an email to an advocate (https://www.facebook.com/groups/314293301959189/1006191742769338/) indicating that the investigators might skip the second exercise test altogether; they certainly, as you said, did not commit to doing the two tests on consecutive days. What’s even more concerning is that the protocol does not seem to include a prior two-day CPET as an entry criterion for the study. Given that this test is about as close to a reliable biomarker as we have, that is highly alarming. Admitting patients into the study based, with respect to PEM, on only subjective questionnaires is a recipe for including people who have do not truly exhibit PEM, but unspecified fatigue instead.
It seems to me that two of the most crucial issues for the study are:
1. Who is doing the study?
2. Who is being studied?
NIH is clearly getting both of these points wrong:
1. NIH is allowing investigators—Walitt, Saligan and Gill—with somatoform/psychosomatic, catastrophizing and GET/CBT biases to influence the study design, day-to-day operations, analysis and conclusions. As you said, these individuals need to be removed as a critical and non-negotiable matter. NIH’s argument that there are checks and balances to protect against bias is not at all reassuring; it is backwards thinking. One would certainly hope that there are investigators within NIH who do not have any bias to start with and our disease deserves that much, at least.
2. NIH is allowing those same biased investigators to have the final say on cohort selection, which is particularly worrisome because (a) as you pointed out, not all "patients will be recruited from well-established ME/CFS clinics,” (b) a two-day CPET is not required to participate in the study and © NIH is planning to use more than one set of criteria.
We have waited over 30 years. Clearly, it is more important to get it right than to proceed prematurely with a study design that is rife with bias and is haphazard at best. NIH owes it to this community to start over with patient and true-expert input in designing the study; followed by a public-comment period; with a single set of criteria (ICC or CCC), a clearly defined patient cohort with a two-day CPET as an entry criterion for the study and the elimination of any biased NIH investigators from the study.
Thank you again for your thorough and important analysis.