
The Chronic Fatigue Syndrome Advisory Committee (CFSAC) provides advice and recommendations to the Secretary of Health and Human Services (HHS) through the Assistant Secretary for Health on issues related to Myalgic Encephalomyelitis and Chronic Fatigue Syndrome (ME/CFS). It meets twice a year.
The last meeting took place August 18 and 19, 2015. The theme of the meeting was HHS’ response to the Institute of Medicine (IOM) and Pathways to Prevention (P2P) reports on redefining ME/CFS. A CFSAC working group was created to work on recommendations for these reports which were presented at the meeting.
Tackling all the recommendations and information provided at the meeting would be too long to include in one blog. Since we believe that the diagnostic and research criteria are a crucial element, we decided to concentrate on the recommendations which reference the criteria.
The Criteria
The 1991 Oxford criteria, published in the U.K., was created to describe both CFS of unknown etiology and a sub-type of CFS called post-infectious fatigue syndrome. This criteria has been used in research for CFS, including in the infamous PACE trial. Because of its inclusiveness and broadness, the research achieved with the Oxford criteria cannot be relied on.
The 1994 CFS Case Definition (Fukuda criteria) was a research criteria proposed by the "International Chronic Fatigue Syndrome Study Group", led by the Centers for Disease Control and Prevention. It demands six months of severe fatigue along with any four of the following eight symptoms to receive a diagnosis of CFS: substantial impairment in short-term memory or concentration; sore throat; tender lymph nodes; muscle pain; multi-joint pain without swelling or redness; headaches of a new type, pattern, or severity; unrefreshing sleep; or post-exertional malaise lasting more than 24 hours.
The 2003 Canadian Consensus Criteria (CCC) was initiated by Health Canada and written by ME/CFS experts. The CCC posits that post exertional malaise and cognitive problems are hallmarks of this disorder and are necessary for a diagnosis. In addition,diagnosis requires two or more neurological/cognitive manifestations and one or more symptoms from at least two of the categories of autonomic, neuroendocrine and immune manifestations, in addition to multiple major criteria of fatigue, post exertional malaise and/or fatigue, chronic pain and sleep dysfunction.
The 2011 International Consensus Criteria (ICC), is the most current criteria created by an international group of ME/CFS experts. This is considered an ME criteria, closest to the one described by Dr. Ramsay in 1956. The six month waiting time for diagnosis is dropped. There is the mandatory symptom of PENE (post exertional neuroimmune exhaustion). It is also accompanied by symptoms from neurological, immune/gastrointestinal/genitourinary, and energy metabolism/transport impairment categories. It demands a reduction of at least 50% of pre-illness activities.
The 2015 Proposed IOM Criteria was created by the Institute of Medicine panel of expert and non-expert professionals. The proposed clinical criteria for diagnosis requires a significant loss of function that persists for six months, post exertional malaise and unrefreshed sleep. In addition, it requires one of two of the following; cognitive impairment or orthostatic intolerance.
History Preceding the Launch of the IOM Criteria
Although there were two newer criteria created (the 2003 CCC and 2011 ICC) since the 1994 Fukuda, the Department of Health and Human services (HHS) persistently insisted on the exclusive use of the outdated, overly broad, Fukuda criteria both for research and diagnostic criteria.
In September 2013,Clinicians, researchers and advocates entreated HHS to recognize and adopt the CCC which was an updated and more accurate criteria for the disease. CFSAC urged HHS to adopt the CCC as well with a recommendation to convene a workshop of ME/CFS stakeholders to work on advising whether it needed any updating. Top ME/CFS researchers started using CCC criteria in addition to the Fukuda criteria for determining patient cohorts. Since the NIH only recognized the Fukuda definition for grant applications, researchers could not just evaluate per the CCC criteria.
HHS did not heed the voice of the community and in 2013 stubbornly and secretly contracted with the IOM to create, yet again, another government supported definition for the disease. This contract was heavily disputed by the great majority of medical specialists as well as patient advocates and patients. Yet, HHS forged ahead and the 2015 IOM criteria was created without guidance on treatments, as instructed by HHS.
Some in the community have accepted the new IOM clinical diagnostic criteria as an improvement to the currently used Fukuda because of its inclusion of the hallmark feature of post-exertional malaise (PEM) as one of the mandatory symptoms. Many others, including MEadvocacy, argue that it actually falls short of the already available CCC and ICC. They feel that this new criteria from the IOM is too broad, inclusive and does not describe the serious neuro-immune disease, myalgic encephalomyelitis.
Why are Case Definitions Consequential?
In the preface to the ICC, its authors explain the need for accurate definitions: “There is a poignant need to untangle the web of confusion caused by mixing diverse and often overly inclusive patient populations in one heterogeneous, multi-rubric pot called ‘chronic fatigue syndrome’. We believe this is the foremost cause of diluted and inconsistent research findings, which hinders progress, fosters skepticism, and wastes limited research monies.”
Some have argued that since the IOM criteria are to be used for clinical diagnostic purposes, and not for research, there is no need for such “tight” criteria. One problem with this line of thought is the fact that the US government has a history of muddling the aim of previous criteria. For example, the Fukuda criteria were created for research purposes yet, they have been used for diagnosis as well.
No request has been made by HHS to come up with new research criteria. Which criteria do you think will be used for federal research going forward? Will they continue to use the inefficient Fukuda? There is evidence, as in Francis Collins’ recent statements of support of the IOM report, that they will start using the new IOM criteria for their research initiatives.
Another complication and confusion will arise when the medical profession starts diagnosing patients with the IOM criteria. Clinicians may observe that many of their ME/CFS patients will have contrasting symptoms or treatment responses compared to the patient populations that are evaluated in the research studies or in other international patient populations such as Canada. Thus, if the research studies find certain treatments successful but the same results are not carried in the clinical settings, the research may be thrown out as uncredible by the medical community.
Incidentally, CFSAC recommendation #4 advocates for the use of the CCC criteria for federally funded research: “CFSAC recommends that federally-funded research specify use of the 2003 Canadian Consensus Criteria as a research case definition for patient selection (in addition to other requirements established for specific research purposes) using standardized and uniform assessment methods and measures for applying the definition.”
The importance of selecting the correct patient group in criteria for the disease has been highlighted in the newest paper by Norwegian scientists titled:‘What exactly is myalgic encephalomyelitis’.The paper states: “The use of broad inclusion criteria has created a heterogeneous patient population, also within research. This has increased the risk of erroneous conclusions, misdiagnosis and incorrect treatment . For myalgic encephalomyelitis, the Canadian criteria and the international consensus criteria have in our view increased the accuracy of diagnosis due to their greater specificity and clearer delineation of the disorder from other forms of fatigue.”
How Well Does The IOM Criteria Select ME Patients?
In his paper ‘Reflections on the IOM's systemic exertion intolerance disease’, ME/CFS researcher, Dr. Leonard Jason, ran an analysis to answer this specific question. In his study of patients who are referred to a specialty clinic and those who self identify to have CFS, the same group was found to have the disease with the IOM criteria as with the Fukuda criteria. Most in this group were already diagnosed as having ME or CFS by clinicians who already accounted for exclusionary conditions. Since the IOM criteria does not require the exclusion of other conditions, a group using IOM criteria will be more inclusive of misdiagnosed patients. Jason’s paper ‘Unintended Consequences of not Specifying Exclusionary Illnesses for Systemic Exertion Intolerance Disease’ suggests that his “findings indicate that many individuals from major depressive disorder illness groups as well as other medical illnesses were categorized as having SEID.”
Frank Twisk published a paper; ‘A Critical Analysis of the Proposal of the IOM to Replace ME and CFS by a New Diagnostic Entity Called SEID’. In the paper, he proposes that some of the characteristic symptoms of ME, as described by Dr. A. Melvin Ramsay, are not present in the IOM criteria. These include muscle fatigability, circulatory impairment and exhaustion of the central nervous system after minor physical activity, as well as the chronic relapsing course of the disease. There are two reasons for these omissions, Frank proposes. 1- These symptoms have not been adequately investigated. (lack of quality research and studies) 2- It is mainly CFS diagnosed patients that have been studied, in the research relied upon [during the IOM’s evidence based evaluation], as opposed to ME patients.
This second point made by Twisk is really key to our subject. If most of the research and studies that the IOM panel relied upon used CFS patients as per Oxford or Fukuda criteria, the resulting criteria will reflect those findings. In essence, the IOM criteria then is a CFS criteria, not ME.
CFSAC Recommendations for Improving the IOM Criteria
Recommendation #4 specifies use of the 2003 CCC criteria be used for any federally-funded research. If this is implemented, the patient population used for research would be a significant improvement over previous studies.
Please read recommendations #8, 9 and 10 to see the details of what CFSAC has added to the IOM criteria. See video of the presentation of these recommendations here.
In her preface to these recommendations, patient advocate and CFSAC voting member, Donna Pearson stressed that the CFSAC working group that created the recommendations did not attempt to “revise” the IOM criteria. Their effort went toward suggesting more details to be included so that the clinician can better diagnose patients. The following recommendations therefore mainly provide for more guidance to be included with the literature of the IOM criteria.
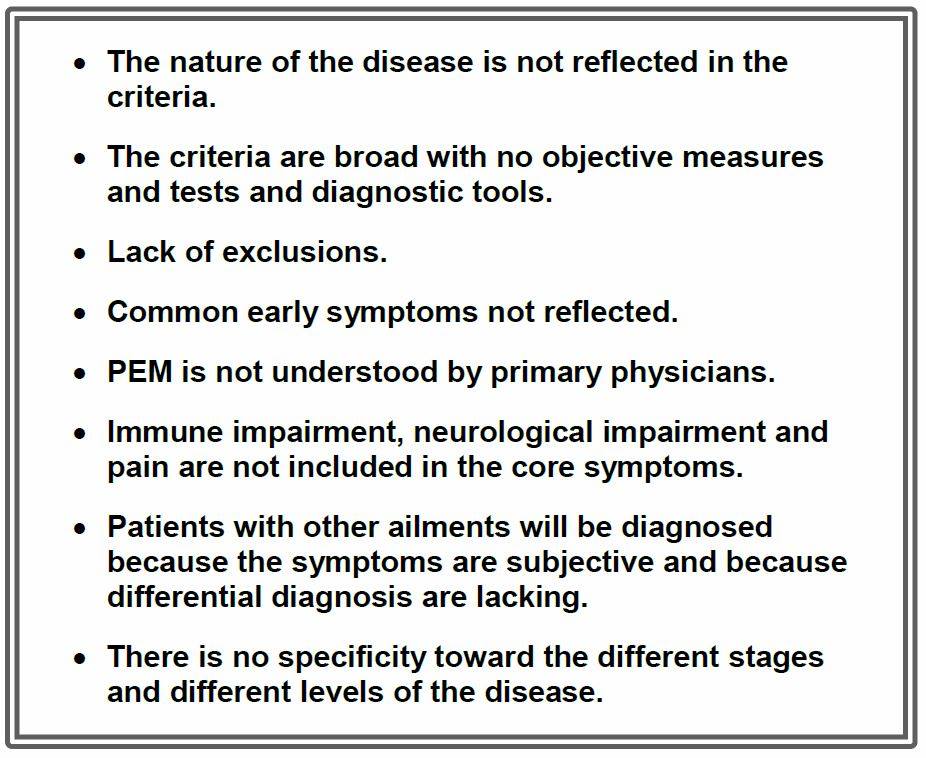
The main concerns that the group found with the IOM criteria were the following:
Recommendation #8 provides for:
-
Inclusion of an “overview” of the disease.
-
Objective testing identified in the IOM report be included.
-
The language “unrefreshed sleep” be changed to “sleep abnormalities”.
-
More descriptive language, from the IOM report, to be included with the core symptoms.
-
Immune dysfunction, neurological dysfunction and pain symptoms among other frequently reported symptoms be reflected with the core symptoms in all materials.
-
The expanded version of the criteria be used in criteria material.
Recommendation #9 advocates for the proposed IOM criteria to be validated and refined if needed within two years by disease experts.
In recommendation #10, the following are suggested to be included in the guidelines:
-
A disease overview including a statement that the disease includes immune, neurological and cognitive impairment, sleep abnormalities, and autonomic dysfunction.
-
Clinical guidelines for assessing post-exertional malaise (PEM).
-
Information about appropriate treatments and care.
-
List of differential diagnosis.
-
List of co-morbid conditions that are experienced with the disease.
-
Statement about the inappropriateness and dangers of cognitive behavior therapy (CBT) and graded exercise treatment (GET) as treatments for this disease.
-
Resource list with links back to the IOM report.
How Does the IOM Criteria Compare to the CCC Criteria?
You can read about the comparison of the IOM and CCC criteria here.
The differences between the two criteria are highlighted in the graphic below:

Will the improvements of CFSAC recommendations to the IOM criteria bring us closer to the CCC criteria?
We commend the CFSAC working group for their monumental achievement in creating all these important recommendations to HHS. Their effort has brought about (if implemented by HHS), many improvements to the IOM criteria and may cause the cohort of diagnosed patients to contain a larger percentage of patients that would meet ME criteria. However, MEadvocacy believes that more needs to be done to bring the IOM criteria in-line with ME criteria.
The one proposed alteration to the actual IOM criteria language by CFSAC was to change “unrefreshed sleep” to “sleep abnormalities”. The other recommendations involved the addition of data, such as explanations how PEM affects ME/CFS patients as well as the additional information of symptoms like immune dysfunction (but not as an inclusion in the core symptoms).The essential list of exclusionary diseases as well as co-morbid manifestations are recommended to be included as well.
A final analysis shows that the CFSAC recommendations are an improvement to the original IOM criteria by the fact that it is more descriptive and includes the much needed list of exclusionary diseases and comorbidities. Unfortunately, it fails in achieving the accuracy of the CCC by not demanding that neurological manifestations, immune dysfunctions and muscle pain be part of the mandatory core symptoms.
Taking Frank Twisk’s analysis into consideration, the IOM criteria (even when improved with the CFSAC recommendations) does not describe the core neuroimmune symptoms of myalgic encephalomyelitis; “(long-lasting) post-exertional muscle fatigue/weakness and signs of cerebral dysfunction”.
Looking Forward to Future Progress
If implemented, the CFSAC recommendation #4 should ensure that going forward, the 2003 CCC will be the sole criteria used for all research. This should technically retire the use of the Oxford and Fukuda criteria for research purposes.
We are hopeful that 2016 will see real progress toward research on patients who have ME. We are excited to see the success and growing support that Dr. Davis’ End ME/CFS Project is experiencing. Their “Giving Tuesday” fundraising effort has come through with over $100,000. In addition, they have received some large private anonymous donations which will definitely make a difference. The Open Medicine Foundation (OMF) has recently announced that due to the generous donations and added knowledge, they have added more tests to the OMF ME/CFS Study.They have uploaded an updated list of tests and an updated full description of the study.
We hope that the next few years will bring biomedical diagnostic criteria that will clean the muddied waters left from the varied poorly defined diagnostic criteria.
What Can You Do?
-
Edit - One Click letter to Congress is no longer available.
-
Help us educate patients so they can become their own advocate by sharing/ liking this blog on social media platforms; liking/and or sharing the MEadvocacy facebook page posts; and liking/retweeting MEadvocacy tweets.
-
Donate to the research of severe ME patients, such as the Open Medicine Foundation (OMF).
Showing 3 reactions
James Frederick
Employed @ http://www.amerangaragedoors.com
what a great post; describes the definition problem with excellent clarity. nicely done gabby.
Also we need to discuss the fact that in essentially all other diseases the professional body does the defining. Why in our disease isn’t the IACFSME deciding? Why instead bring in a majority who have never seen a patient?